‘S’ is also for ‘scanxiety’.

In 1935 Austrian physicist Erwin Schrodinger developed a thought experiment in order to stimulate discussion around the widely accepted but problematic Copenhagen interpretation of quantum mechanics. The Copenhagen interpretation posits that physical systems do not have definite properties until they are observed and measured. Once observed and measured, the system ‘collapses’ into one or other of the possible ‘definite’ states. So it’s kind of like a sciencey take on the old philosophical conundrum ‘if a tree falls in the woods and no-one hears it, does it make a sound?’.
But as Schrodinger was a physicist not a philosopher, he wanted to point out the apparent absurdity of the Copenhagen interpretation and so created his famous thought experiment, which ran thus:
Put a cat (a theoretical one, not a real live fluffy kitty, even 1930s scientists had boundaries) in a steel box with a Geiger counter, a tiny amount of radioactive substance and a vial of poison. The amount of the radioactive substance is so small that there’s a chance an atom of it may, or may not, decay inside an hour. If it does decay then it will set off the Geiger counter, which will trigger a hammer to break the vial of poison and kill the cat (poor kitty). If it doesn’t decay, the vial will remain unbroken and the cat will stay alive (yay kitty). According to the Copenhagen interpretation, as physical systems only have definite properties once observed and measured, the cat is both dead and alive in the box until it is opened and the deadness or aliveness of the cat is observed. (Deadness and aliveness being genuine sciencey terms).
And there endeth my lesson in theoretical physics. The full extent of my knowledge in which was gained from my physics A level (grade C), a quick skim of Wikipedia and binge-watching ‘The Big Bang Theory’. Although tbh I’m not even sure the above is 100% accurate, but as I don’t think there are quantum scientists in my friendship group, I might get away with it.
But you’re probably asking ‘why on earth is Karen wittering on about quantum mechanics? Where are the gory stories about blood spattered boobs? That’s what we came here for!’. Well, Schrodinger’s ‘dead or alive cat’ theory has been reduced by popular culture from a highly complex discussion about physical theorems to a basic meme about uncertainty and it came squarely to mind as I waited the three weeks after my re-excision surgery for the latest pathology results.
Because until you’re in the doctor’s office, until they’ve looked you square in the face and told you those results, then two possibilities are simultaneously alive and running riot in your head. One – the re-excision surgery did what it was supposed to do and there are no cancerous cells left in your breast tissue. Two – the repeat surgery did not succeed and there are still cancerous cells waiting to mutate and invade. Like the unfortunate cat, until you have stepped over the threshold into that locked steel box, and the surgeon’s given you the equivalent of either the decaying atom or the non-decaying atom, there is the potential for good news and bad news, both possibilities exist at the same time. The vial of poison will break. Or will not break. Like poor old puss, your hopes and wishes are simultaneously alive and dead.
Why, I hear you ask (you guys are asking a lot today), is the result of a cancer test any different to any other medical test? Well, of course, in truth it’s not. Every test result has the possibility of bringing relief or gloom. But for the majority of healthy people undergoing tests to rule out medical conditions, there’s a good chance that the odds are going to be stacked in your favour. Serious health conditions that require urgent or continuing treatment affect, thank goodness, a fairly small proportion of the population. But when you’ve had a cancer diagnosis (or that of any other chronic, serious or life-threatening condition) you’ve already fallen foul of the odds. 1 in 8 women will be diagnosed with breast cancer in their lifetime. 1 in 8. That’s 12.5% of women. And I managed to be that 1 out of 8, stuck in that sucky 12.5% rather than in that wonderful, lucky 87.5%. So you know you’ve failed in the luck of the draw once. And when the cancer anxiety-worm gets in your brain, it starts whispering all sorts of things. ‘Well, if you were stupid enough to be that 1 in 8, then you’re probably also stupid enough to be in the 43% of women with breast cancer for whom breast conserving surgery doesn’t work’*.
And thanks to that ear-worm, test results become a huge source of anxiety. Waiting becomes painful, time slows to a crawl, a day feels like a week even when you’re able to distract yourself with the necessary minutae of everyday life, and in the special hell of a hospital waiting room an hour feels like a month of intense, stomach-churning agony. In the cancer world, there’s even a word for the creeping panic that comes from waiting for test results, especially for the post-treatment mammograms that breast cancer survivors endure every year. That word is ‘scanxiety’.
So on Wednesday 19 September 2018 I was enduring severe ‘scanxiety’ as I waited to see my surgeon for my second post-op pathology results. There had already been one aborted attempt to get these results the week before, when after yet another agony of waiting I saw my less-than-ideal surgeon only to be told they weren’t ready yet. Deflated and distressed by the delay, it didn’t help that the my lovely ‘oh so switched on to how people feel’ surgeon, explained the delay by detailing how the tissue they cut out of you can be too ‘jellified’ to test properly and how they have to wait for it to ‘firm up’ before it can be sliced into proper slivers to examine. Because what I needed right then was a mental image of my excised boob tissue turning from jelly to solid on a plate before being hacked into pieces. Yep.
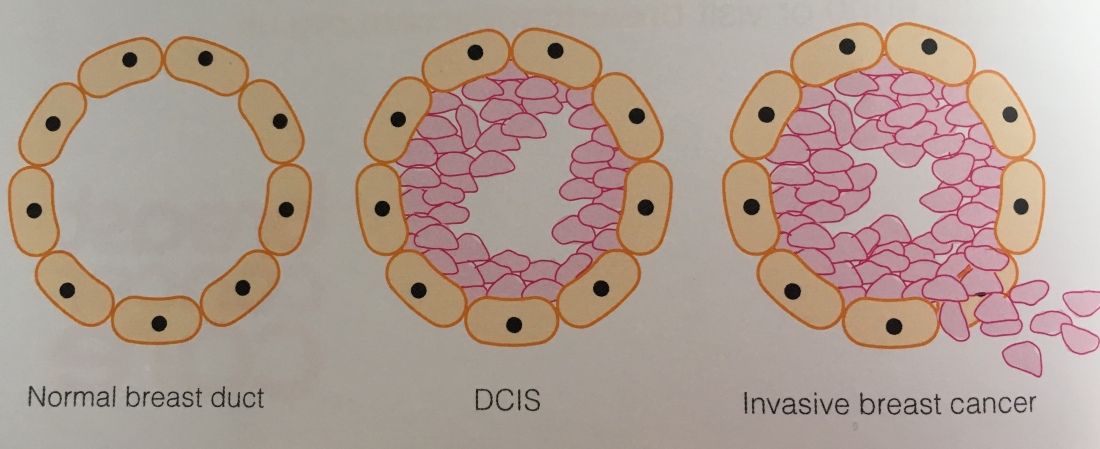
After that glorious encounter in my litany of surgeon faux-pas, the appointment on 19 September was always going to be high on the stress-o-meter. And the news I was given didn’t alleviate any of that. Unfortunately, my surgeon said, the re-excision surgery had still failed to get clear margins. There was still evidence of DCIS (cancerous cells currently contained within ducts in my breast) up to the margins of the tissue removed. This meant that there was still DCIS present in the remaining breast tissue. And that meant there was really only one option. A mastectomy.
I thought the bottom had fallen out of my world when I was given the original cancer diagnosis. But because I had been reassured that minimal surgery and radiotherapy would probably be enough to treat the cancer, I had felt confident that I could tackle it head on. To jump from that to the position where I was going to lose all of an intimate part of my anatomy to a surgeon’s scalpel was more than my brain could deal with. I fogged out the rest of the conversation and it was only when I moved to another room with a good friend by my side (mwah to her!) and my Breast Care Nurse, that I let the wall of emotion hit me. Tears flooded out. Angry, scared, confused, bewildered tears. Six weeks ago I’d thought I’d be doing a quick ‘1-2-3’ (see U is for ‘understanding’) to the end of treatment but now it seemed to have turned into a ‘1-repeat 1-repeat much bigger 1’. My BCN said she always felt sorry for women with DCIS who were suddenly confronted with a mastectomy, because they were often told that it was the ‘best kind of breast cancer to have’ and that it was treatable with simple surgery, but then had to readjust to the news that they’d actually need to lose a body part for that treatment to work.
And that is what’s next on the cards for me. A major piece of surgery that will carve away a huge part (well, maybe not huge but at least a good handful) of the body that I’ve grown and grown into my entire life. I can honestly tell you that now, over 7 weeks since I first heard that devastating news, I still haven’t processed it, understood it, dealt with it, accepted it. There’s a blog post to come about what a mastectomy is, what surgery and recovery looks like and what a woman’s options for reconstruction are but even now I know I won’t be able to explain or articulate how it feels to know that’s what my future holds.
* statistics from Breast Cancer Care: https://www.breastcancercare.org.uk/sites/default/files/files/breast-cancer-stats-sheet-february-2015.pdf